

美国医疗不平等早已有之,近期则更加严重
Sy Mukherjee
2020-06-25
美国有色人种,尤其是黑人,长期承受着医疗服务的不平等。
 文本设置
文本设置
 Plus(0条)
Plus(0条) 

人们很容易认为新冠病毒不搞种族歧视。毕竟,这是种病原体,是一种病毒。病毒感染宿主,传播过程中并不区分传染对象。
但数字却告诉我们并非如此,真实的故事令人沮丧——有色人种,尤其是美国黑人,长期承受着医疗服务的不平等,如今的新冠疫情不过是历史的延续。
新冠病毒的种族难题
新冠病毒对美国黑人的影响更大。过去几个月的疫情证明了这个基本事实。根据新冠追踪项目(COVID Tracking Project)对不同种族数据的调查,尽管黑人仅占美国人口的13%,但在已知其族裔的新冠病毒死亡病例中,近四分之一是黑人。
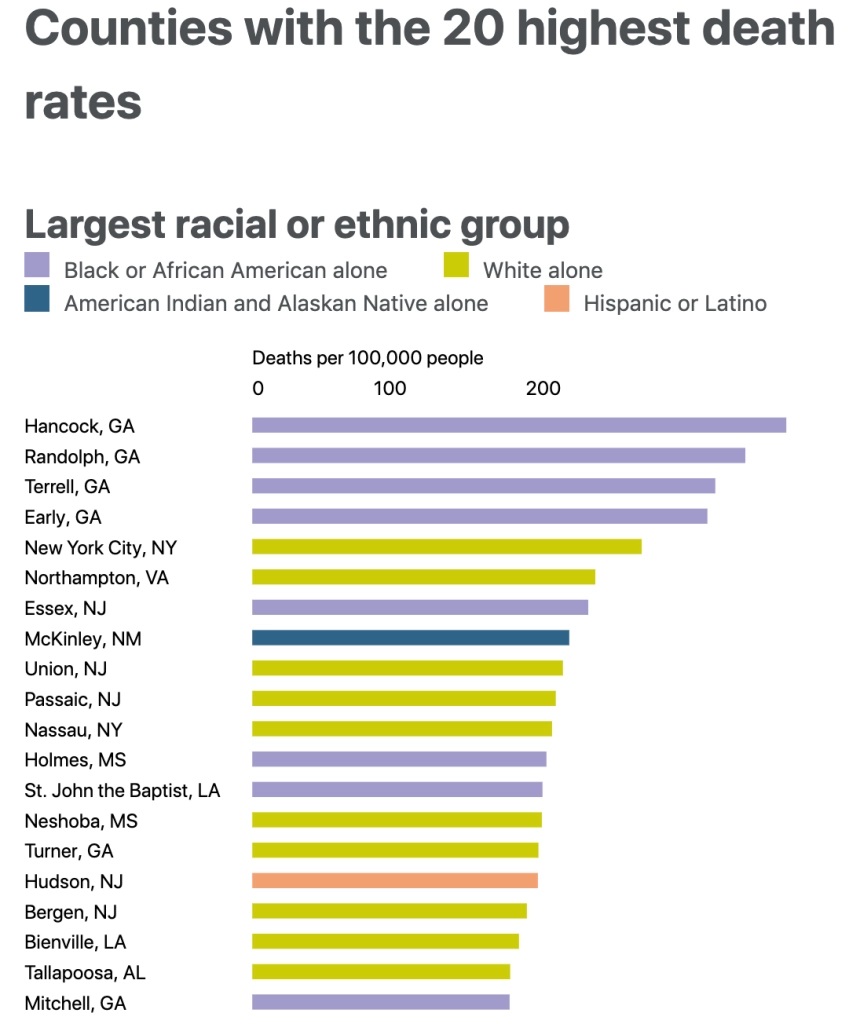
在美国新冠病毒致死率最高的20个县中,有8个是以黑人为主的地区。
调查还显示出本次危机的影响之广。“你可以看到,这些差异在新冠危机期间尤为明显,”珍妮弗·本茨说,她是芝加哥大学美联社-NORC公共事务研究中心的首席研究科学家和副主任。“我们用来调查种族和民族差异的一项重要举措是,询问受访者是否有家人或密友死于新冠病毒。不同种族之间的差异非之大,令人难以置信。”
全美接受调查的白人中,约有4%的人有认识的人死于新冠,而在黑人中,这一比例为11%。新冠追踪项目的数据显示,地区和地区之间也有不同,在某些地区,种族差异甚至更加惊人。在亚特兰大,4%的白人和14%的黑人有认识的人死于新冠。巴尔的摩的比例也差不多,伯明翰的情况则更糟。
造成这些明显差异的确切原因尚不清楚。在某种程度上,基因可能会产生一定影响。但起作用的还有无数其他因素。
“如果人们有基础病,感染新冠肺炎的后果会更糟。数十年的研究表明,美国黑人患心脏病、糖尿病、高血压和其他类似疾病的比例过高。”本茨说,“然后你就会看到,所有这些长期存在的不平等如何在新冠谜题中拼在一起。”
医疗不平等总是祸不单行
“先天与后天”的争论已经持续了几十年。如果有人得了心脏病或其他慢性疾病,这是他们自己的错吗,表面上看起来是因为他们选择吃不健康的食物、吸烟、喝酒、不锻炼?还是说,这是一个由于多年系统性不平等造成的复杂问题?
非营利性的健康巨头凯撒医疗集团(Kaiser Permanente)的已故首席执行官伯纳德·泰森是“健康的社会决定因素”理论的热心传播者,该理论将责任归咎于系统性不平等。
“我们认为,很多可能不会归类到‘医疗保健’这个项目下的元素会对人们的健康福祉产生直接影响,他们是整个健康生态系统的一部分。”泰森在他猝然辞世前一年,曾经向《财富》杂志说道。“我们现在知道,健康的社会决定因素指的是归类到其他领域而我们还没有切实解决的很多问题,他们对一个人健康的影响远远超过医疗保健本身。邮政编码是其中最重要的因素之一。这一点也不夸张,你可以看到一个地区和另一个地区预期寿命间存在差异。”
“一个人的邮政编码可以很好地预测他们未来的健康状况。这不仅仅是个人的选择,而且是由一个人所处的生活环境和政策结构决定的。”本茨补充道。
邮政编码不同意味着,你可能生活在一个超市里有足量新鲜农产品的地方,也可能是一个必须依靠街角商店或杂货店获得营养的食物沙漠。社会经济机会的缺乏或许意味着能在家做饭和不得不上夜班之间的差别。美国环境保护署(Environmental Protection Agency)在2018年的一项分析发现,黑人暴露在PM2.5中的“负担要高出1.54倍”,而PM2.5是化石燃料燃烧产生的一种空气污染物,会对心脏病、肺病和寿命缩短产生影响。
在新冠疫情时代,这些因素共同作用,导致了明显的不平等现象。
医疗歧视的历史早已有之
在乔治·弗洛伊德被一名白人警察杀害后,美国人急剧转向支持“黑人的命也是命”(Black Lives Matters)运动。《财富》杂志和德勤(Deloitte)对222名首席执行官进行的调查显示,62%的首席执行官正计划在公司推出切实政策,回应当前的抗议和动荡。
随着各州重新开放,新冠病毒病例再次增加,一些官员称在“黑人的命也是命”抗议活动中,人们忽视社交距离,对新冠传播产生了影响。官员们鼓励抗议者保持距离,戴上口罩,并在参加团体活动后进行检测——但美国黑人不大可能有机会接受检测。同样不清楚的是,在露天抗议中,人们戴着口罩或保持一定距离,并采取了其他预防措施,这与在封闭空间中不戴口罩产生的结果是否一样。
然而,公众因为警察暴行意识到了系统性种族主义的存在,这个认识似乎并未延伸到医疗领域。
“很多美国人甚至没有意识到医疗服务中存在种族差异。”本兹说。芝加哥大学的NORC中心在21世纪初和2010年代进行了一系列研究,发现超过70%的受访者认为,在与警察打交道时,黑人比白人受到了更不公平的对待,而只有42%的受访者认为在获取医疗服务方面存在同样问题。
有多项研究描绘出了一个不同的现实。美国黑人获得医疗服务的机会一直在减少,而且即便他们得到了医疗服务,也往往是不合格的服务,或者会由于陈腐的刻板印象和交流障碍而面临歧视。
“医生需要使用集群信息做出诊断和其他复杂的判断,而且往往没有足够多时间和资源收集所有相关信息就必须作出判断。”美国医学研究所理解并消除医疗族裔差异委员会(the Institute of Medicine (US) Committee on Understanding and Eliminating Racial and Ethnic Disparities in Health Care)
在一份影响广泛的报告写道,“时间压力和资源不足的情况在临床治疗中很常见,并且和那些由于信息不足、刻板印象和偏见产生的负面结果密切相关。”
约翰斯·霍普金斯大学的另一项独立研究得出结论:“开设培训项目,提升处理情绪问题、建立融洽关系的沟通技能,有望减少医疗方面的种族差异,提升少数族裔患者的信任。”
换句话说,一个以白人医生为主的医生团队并不一定知道与黑人病人互动的最佳方式,这就导致了信任的根本性缺失,而信任正是医疗决策的核心。
然后是医保本身的覆盖问题。虽然《平价医疗法案》(Affordable Care Act,又称奥巴马医改)大幅提高了为美国穷人或残疾人提供保险的医疗补助计划(Medicaid)等政府项目的规模,但它的福利是不对称的。各州有权根据法律选择是否扩大医疗补助计划。根据无党派的凯泽家庭基金会(Kaiser Family Foundation)的数据,少数几个没有扩展医疗补助计划的州往往是南方的贫困州,这对有色人种社区有巨大影响。
还有230万美国人陷入了所谓的“保险缺口”,他们赚的钱刚好不够资格申请医疗补助计划,但又不够多,无法获得奥巴马医改(Obamacare)为个人私人保险计划提供的补贴。
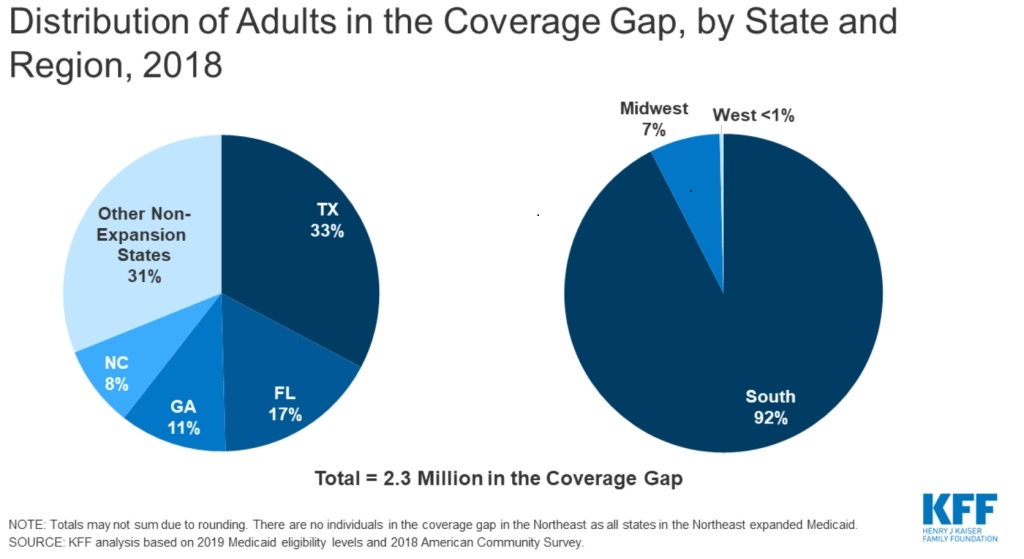
拥有大量黑人人口的南部州,特别是得克萨斯州和佛罗里达州,保险覆盖的缺口最大。
新冠病毒大流行带来的金融灾难显然让问题雪上加霜。近一半美国人通过雇主获得医疗保险,将医保和工作绑定是一系列历史事件的结果。
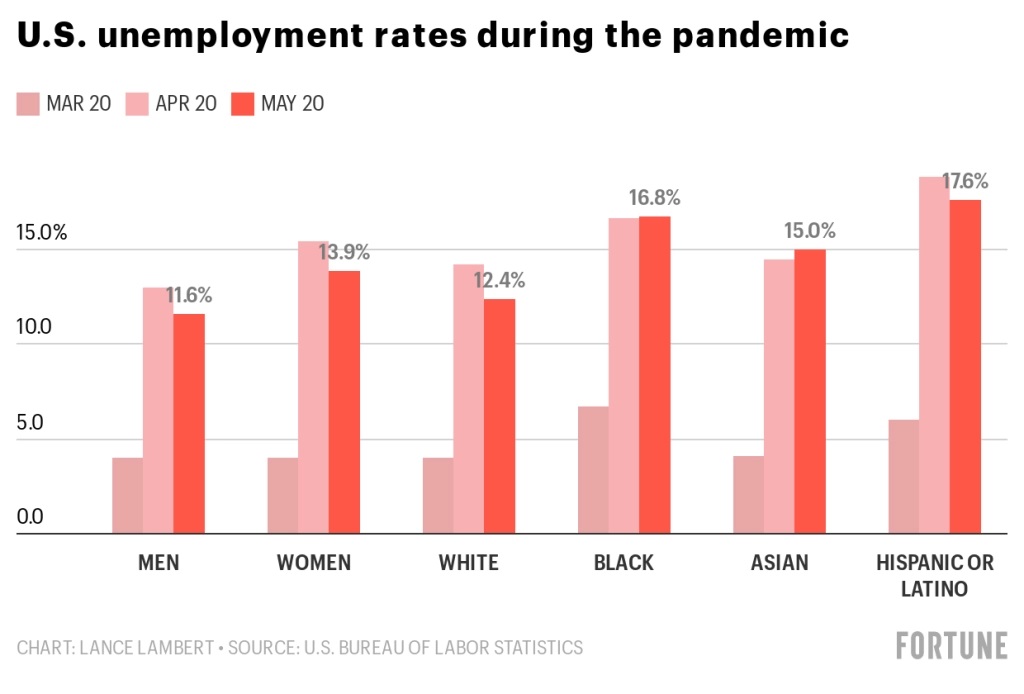
最新的联邦就业报告显示,美国黑人,尤其是黑人女性,在失业危机中首当其冲。5月,白人的失业率从14.2%降至12.4%,而黑人的失业率则从16.7%升至16.8%。
毫无疑问,健康是选择和机会共同作用的结果。我们的生物机制产生的结果可能是随机的,这不是任何人的错。但对许多美国黑人来说,很早之前,别人就代他们做出了“选择”。(财富中文网)
译者:Agatha
人们很容易认为新冠病毒不搞种族歧视。毕竟,这是种病原体,是一种病毒。病毒感染宿主,传播过程中并不区分传染对象。
但数字却告诉我们并非如此,真实的故事令人沮丧——有色人种,尤其是美国黑人,长期承受着医疗服务的不平等,如今的新冠疫情不过是历史的延续。
新冠病毒的种族难题
新冠病毒对美国黑人的影响更大。过去几个月的疫情证明了这个基本事实。根据新冠追踪项目(COVID Tracking Project)对不同种族数据的调查,尽管黑人仅占美国人口的13%,但在已知其族裔的新冠病毒死亡病例中,近四分之一是黑人。
在美国新冠病毒致死率最高的20个县中,有8个是以黑人为主的地区。
调查还显示出本次危机的影响之广。“你可以看到,这些差异在新冠危机期间尤为明显,”珍妮弗·本茨说,她是芝加哥大学美联社-NORC公共事务研究中心的首席研究科学家和副主任。“我们用来调查种族和民族差异的一项重要举措是,询问受访者是否有家人或密友死于新冠病毒。不同种族之间的差异非之大,令人难以置信。”
全美接受调查的白人中,约有4%的人有认识的人死于新冠,而在黑人中,这一比例为11%。新冠追踪项目的数据显示,地区和地区之间也有不同,在某些地区,种族差异甚至更加惊人。在亚特兰大,4%的白人和14%的黑人有认识的人死于新冠。巴尔的摩的比例也差不多,伯明翰的情况则更糟。
造成这些明显差异的确切原因尚不清楚。在某种程度上,基因可能会产生一定影响。但起作用的还有无数其他因素。
“如果人们有基础病,感染新冠肺炎的后果会更糟。数十年的研究表明,美国黑人患心脏病、糖尿病、高血压和其他类似疾病的比例过高。”本茨说,“然后你就会看到,所有这些长期存在的不平等如何在新冠谜题中拼在一起。”
医疗不平等总是祸不单行
“先天与后天”的争论已经持续了几十年。如果有人得了心脏病或其他慢性疾病,这是他们自己的错吗,表面上看起来是因为他们选择吃不健康的食物、吸烟、喝酒、不锻炼?还是说,这是一个由于多年系统性不平等造成的复杂问题?
非营利性的健康巨头凯撒医疗集团(Kaiser Permanente)的已故首席执行官伯纳德·泰森是“健康的社会决定因素”理论的热心传播者,该理论将责任归咎于系统性不平等。
“我们认为,很多可能不会归类到‘医疗保健’这个项目下的元素会对人们的健康福祉产生直接影响,他们是整个健康生态系统的一部分。”泰森在他猝然辞世前一年,曾经向《财富》杂志说道。“我们现在知道,健康的社会决定因素指的是归类到其他领域而我们还没有切实解决的很多问题,他们对一个人健康的影响远远超过医疗保健本身。邮政编码是其中最重要的因素之一。这一点也不夸张,你可以看到一个地区和另一个地区预期寿命间存在差异。”
“一个人的邮政编码可以很好地预测他们未来的健康状况。这不仅仅是个人的选择,而且是由一个人所处的生活环境和政策结构决定的。”本茨补充道。
邮政编码不同意味着,你可能生活在一个超市里有足量新鲜农产品的地方,也可能是一个必须依靠街角商店或杂货店获得营养的食物沙漠。社会经济机会的缺乏或许意味着能在家做饭和不得不上夜班之间的差别。美国环境保护署(Environmental Protection Agency)在2018年的一项分析发现,黑人暴露在PM2.5中的“负担要高出1.54倍”,而PM2.5是化石燃料燃烧产生的一种空气污染物,会对心脏病、肺病和寿命缩短产生影响。
在新冠疫情时代,这些因素共同作用,导致了明显的不平等现象。
医疗歧视的历史早已有之
在乔治·弗洛伊德被一名白人警察杀害后,美国人急剧转向支持“黑人的命也是命”(Black Lives Matters)运动。《财富》杂志和德勤(Deloitte)对222名首席执行官进行的调查显示,62%的首席执行官正计划在公司推出切实政策,回应当前的抗议和动荡。
随着各州重新开放,新冠病毒病例再次增加,一些官员称在“黑人的命也是命”抗议活动中,人们忽视社交距离,对新冠传播产生了影响。官员们鼓励抗议者保持距离,戴上口罩,并在参加团体活动后进行检测——但美国黑人不大可能有机会接受检测。同样不清楚的是,在露天抗议中,人们戴着口罩或保持一定距离,并采取了其他预防措施,这与在封闭空间中不戴口罩产生的结果是否一样。
然而,公众因为警察暴行意识到了系统性种族主义的存在,这个认识似乎并未延伸到医疗领域。
“很多美国人甚至没有意识到医疗服务中存在种族差异。”本兹说。芝加哥大学的NORC中心在21世纪初和2010年代进行了一系列研究,发现超过70%的受访者认为,在与警察打交道时,黑人比白人受到了更不公平的对待,而只有42%的受访者认为在获取医疗服务方面存在同样问题。
有多项研究描绘出了一个不同的现实。美国黑人获得医疗服务的机会一直在减少,而且即便他们得到了医疗服务,也往往是不合格的服务,或者会由于陈腐的刻板印象和交流障碍而面临歧视。
“医生需要使用集群信息做出诊断和其他复杂的判断,而且往往没有足够多时间和资源收集所有相关信息就必须作出判断。”美国医学研究所理解并消除医疗族裔差异委员会(the Institute of Medicine (US) Committee on Understanding and Eliminating Racial and Ethnic Disparities in Health Care)
在一份影响广泛的报告写道,“时间压力和资源不足的情况在临床治疗中很常见,并且和那些由于信息不足、刻板印象和偏见产生的负面结果密切相关。”
约翰斯·霍普金斯大学的另一项独立研究得出结论:“开设培训项目,提升处理情绪问题、建立融洽关系的沟通技能,有望减少医疗方面的种族差异,提升少数族裔患者的信任。”
换句话说,一个以白人医生为主的医生团队并不一定知道与黑人病人互动的最佳方式,这就导致了信任的根本性缺失,而信任正是医疗决策的核心。
然后是医保本身的覆盖问题。虽然《平价医疗法案》(Affordable Care Act,又称奥巴马医改)大幅提高了为美国穷人或残疾人提供保险的医疗补助计划(Medicaid)等政府项目的规模,但它的福利是不对称的。各州有权根据法律选择是否扩大医疗补助计划。根据无党派的凯泽家庭基金会(Kaiser Family Foundation)的数据,少数几个没有扩展医疗补助计划的州往往是南方的贫困州,这对有色人种社区有巨大影响。
还有230万美国人陷入了所谓的“保险缺口”,他们赚的钱刚好不够资格申请医疗补助计划,但又不够多,无法获得奥巴马医改(Obamacare)为个人私人保险计划提供的补贴。
拥有大量黑人人口的南部州,特别是得克萨斯州和佛罗里达州,保险覆盖的缺口最大。
新冠病毒大流行带来的金融灾难显然让问题雪上加霜。近一半美国人通过雇主获得医疗保险,将医保和工作绑定是一系列历史事件的结果。
最新的联邦就业报告显示,美国黑人,尤其是黑人女性,在失业危机中首当其冲。5月,白人的失业率从14.2%降至12.4%,而黑人的失业率则从16.7%升至16.8%。
毫无疑问,健康是选择和机会共同作用的结果。我们的生物机制产生的结果可能是随机的,这不是任何人的错。但对许多美国黑人来说,很早之前,别人就代他们做出了“选择”。(财富中文网)
译者:Agatha
It's tempting to think that the coronavirus pandemic sees no color. This is, after all, a pathogen. A virus. A virus infects a host, and it spreads with no regard for who or what unto it may latch.
But the numbers tell a different story—a tale that's a depressing continuation of longstanding health care disparities for people of color in general and black Americans in particular.
The racial COVID conundrum
COVID-19 has a disproportionate impact on black Americans. That's a basic reality that's become clear over the past few months of the pandemic. While black people constitute just 13% of the U.S. population, nearly one in four COVID-19 deaths where the patient's race is known is black, according to the COVID Tracking Project's racial data initiative.
Surveys underscore how much further the crisis extends. "You see these disparities play out particularly acutely during the COVID crisis," says Jennifer Benz, principal research scientist and deputy director of The Associated Press-NORC Center for Public Affairs Research at the University of Chicago. "One of our key measures that illustrates the racial and ethnic disparities is asking people if they have a family member or close friend who they know has died from COVID. And the differences are incredibly stark."
Across the U.S., about 4% of white Americans surveyed know somebody who's died from COVID-19 versus 11% of black Americans. It can vary from region to region, and the disparity is even larger in certain areas as reflected in the COVID Tracking Project data. In Atlanta, 4% of whites versus 14% of blacks know someone who has died from COVID. The figures are similar in Baltimore and even worse in Birmingham.
The precise reason for these stark disparities is nebulous. Genetics may play a part, to an extent. But numerous other factors may come into play.
"The outcomes are so much worse when people have other pre-existing conditions. Decades of research have shown the disproportionate rate at which black Americans have heart disease, diabetes, hypertension, and other such conditions," says Benz. "And then you begin to see how all these longstanding inequities fit together in the puzzle that is COVID."
A perfect storm of health inequities
The "nature versus nurture" debate has raged for decades. If someone develops heart disease or another chronic condition, is it their fault because they ostensibly chose to eat unhealthy foods, smoke cigarettes, drink alcohol, or not exercise? Or is that a far more complicated issue that stems from years of systemic inequities?
Bernard Tyson, the late CEO of nonprofit health giant Kaiser Permanente, was an ardent evangelist for the theory of the "social determinants of health" which lays significant blame on the latter proposition.
"We think all the ingredients are in place to move into other lanes that are directly linked to the health and wellbeing of people that would not fit neatly under the category of ‘health care,’ but that are part of the whole ecosystem of health," he told Fortune a year before his untimely death. "And we now know that the social determinants of health—many of the other categories that we haven’t really addressed concretely—impact a person’s health much more than medical care. One of the big ones is the thing called the zip code. Literally, you can see the differences in the life expectancy in one zip code versus another."
"Somebody's zip code can be so predictive of what health outcomes they face. It's not just individual choices, but one's environment and the policy structures within which they live their lives," adds Benz.
A zip code can mean the difference between living in a region with abundant access to supermarkets that sell fresh produce versus food deserts where one must rely on a corner store or bodega for nutrition. A lack of socioeconomic opportunity may spell the difference between being able to prepare a home cooked meal or working the graveyard shift. A 2018 Environmental Protection Agency (EPA) analysis found that black people "had 1.54 times higher burden" in exposure to PM 2.5, an air pollutant created by burning fossil fuels that's linked with heart disease, lung disease, and generally shorter life spans.
In the COVID era, these are all factors that play into the inequities clearly on display.
A persisting history of medical discrimination
Americans have swung sharply in support of the Black Lives Matter movement in the wake of George Floyd's killing by a white police officer. A survey by Fortune and Deloitte of 222 CEOs found that 62% of the chief executives are planning tangible policy challenges in their workplaces as a response to the protests and unrest.
Coronavirus cases have risen as states reopen, and some officials have pointed to the impact of the socially undistanced Black Lives Matters protests. Officials have encouraged protestors to isolate, wear masks, and get tested after attending group events—but black Americans are less likely to have access to testing facilities. It's also unclear whether or not an open air protest where people are properly masked or distanced and taking other precautions is nearly as much of a problem as being in enclosed spaces unmasked.
The public cognizance of systemic racism when it comes to police brutality, though, doesn't appear to extend to medicine.
"A lot of Americans aren't even aware that these disparities in health care exist," says Benz. University of Chicago's NORC conducted a series of studies in the early 2000s and 2010s finding that while more than 70% of respondents believed black people were treated more unfairly than white people when it came to interactions with police, just 42% said the same of access to health care.
Multiple studies paint a different reality. Black Americans consistently face fewer opportunities to get medical care and, even if they do, tend to receive substandard care or face discrimination based on antiquated stereotypes and communication barriers.
"Physicians use clusters of information in making diagnostic and other complex judgments that must be arrived at without the luxury of the time and other resources to collect all the information that might be relevant," reads a sweeping report by the Institute of Medicine (US) Committee on Understanding and Eliminating Racial and Ethnic Disparities in Health Care. "These conditions of time pressure and resource constraints are common to many clinical encounters, and map closely onto those identified as producing negative outcomes due to lack of information, to stereotypes, and to prejudice."
A separate study from Johns Hopkins concludes that "communication skills training programs targeting emotion-handling and rapport-building behaviors are promising strategies to reduce disparities in health care and to enhance trust among ethnic minority patients."
In other words: A largely white physician force doesn't necessarily know the best ways to interact with black patients, and that leads to an inherent dearth of trust—the beating heart of medical decision-making.
And then there's access to health care itself. While the Affordable Care Act, also known as Obamacare, significantly ramped up government programs such as Medicaid, the insurance option for poor or disabled Americans, its benefits were asymmetric. States had the option to choose to expand Medicaid under the law. The few states which have not expanded Medicaid tend to be poor states in the South, which has an outsize effect on communities of color, according to the nonpartisan Kaiser Family Foundation.
Then there were the 2.3 million Americans who fell into the so-called "coverage gap" where they made just enough money not to qualify for Medicaid but not quite enough to receive Obamacare's subsidies for individual private plans.
Southern states with large black populations, particularly Texas and Florida, have some of the biggest gaps in coverage.
The financial catastrophe wrought by the coronavirus pandemic certainly hasn't made things easier. Nearly half of Americans receive health insurance through their employer, a result of a series of historical accidents which have linked insurance to having a job.
The most recent federal jobs report found that black Americans, and black women in particular, have borne the brunt of the unemployment crisis. While the unemployment rate dipped from 14.2% to 12.4% for white people in May, it rose from 16.7% to 16.8% for black people.
There's no doubt that health is based on a combination of choice and chance. Our biological machinery can lead to arbitrary outcomes which are the fault of no one. But for many black Americans, the "choices" were made by others on their behalf long ago.
请打开财富Plus APP